Chemistry Panel (SMAC 25)
Blood Test for Fatigue and Nutritional Deficiencies
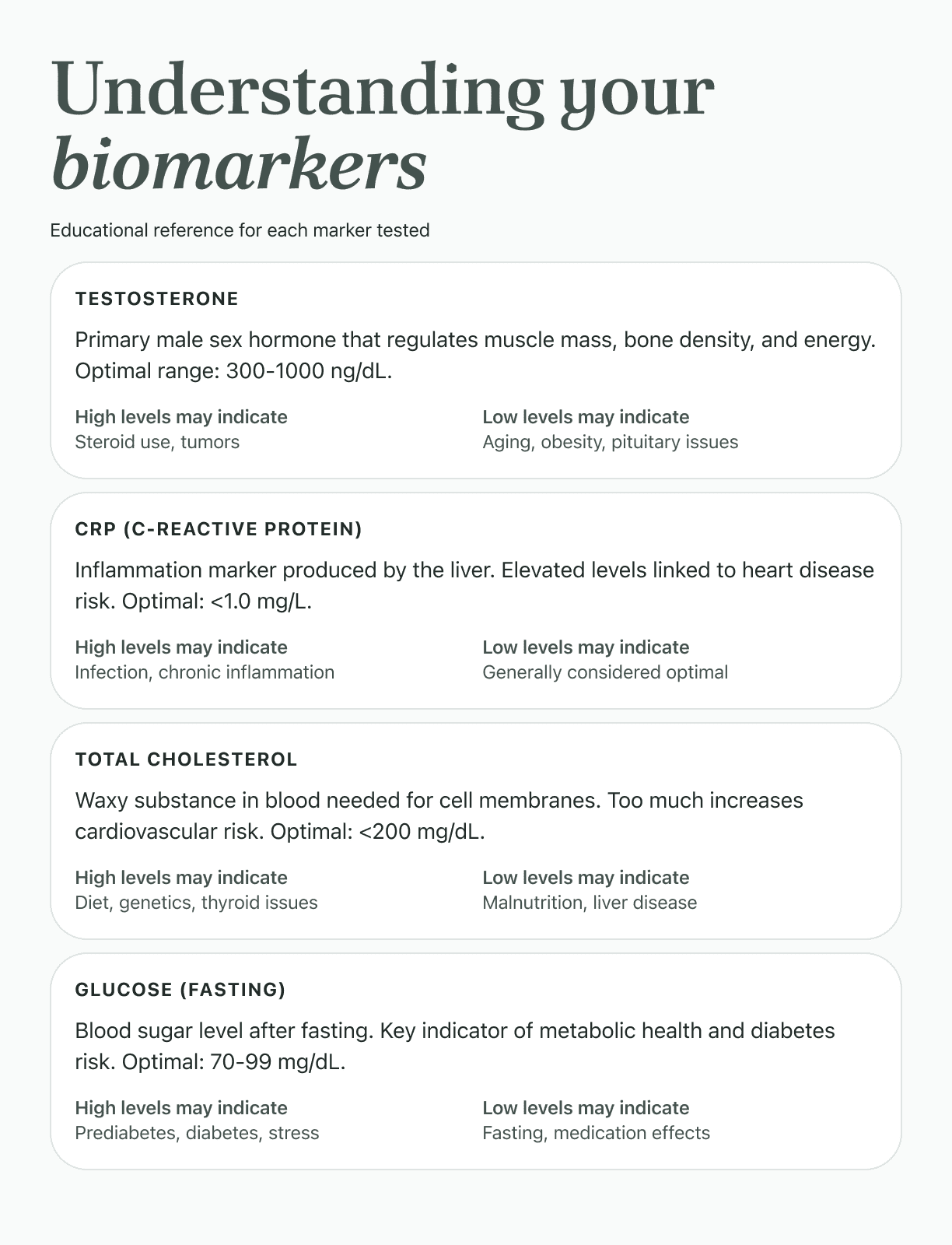
What this test measures
Chloride
Hyperchloremia frequently develops in AKI due to reduced renal chloride excretion and fluid resuscitation with chloride-rich solutions (0.9% saline). Chloride monitoring guides fluid management and helps assess renal recovery.
Potassium
Acute adrenal insufficiency causes severe hyperkalemia with hyponatremia and hypoglycemia. Electrolyte pattern helps diagnose this life-threatening emergency requiring immediate corticosteroid replacement.
Sodium
Hyponatremia results from aldosterone deficiency causing renal sodium loss and cortisol deficiency impairing water excretion. Sodium is a key diagnostic marker in primary adrenal insufficiency.
Bun/Creatinine Ratio
A high BUN/Creatinine ratio can indicate conditions such as kidney disease or dehydration, as both BUN and creatinine are waste products filtered by the kidneys.
ALT
Elevated ALT levels can indicate liver damage, as ALT is an enzyme found primarily in the liver.
AST
High levels of AST can also indicate liver damage, as it is an enzyme that is often released when the liver is injured.
Alkaline Phosphatase
High levels of alkaline phosphatase can indicate liver disease or bone disorders, as this enzyme is produced in both the liver and bones.
Bilirubin, Total
Massive hepatocellular necrosis from acetaminophen overdose causes markedly elevated total bilirubin. Rising bilirubin indicates fulminant hepatic failure and poor prognosis.
Albumin/Globulin Ratio
An abnormal albumin/globulin ratio can indicate liver disease. The liver produces albumin and globulin, so changes in their levels might point to liver dysfunction.
Globulin
High levels of globulin can indicate certain infections, autoimmune diseases, and blood disorders, as globulin proteins are part of the body's immune response.
Albumin
Chronic CHF causes hypoalbuminemia through hepatic congestion impairing synthesis, intestinal edema reducing absorption, and cardiac cachexia. Low albumin (<3.5 g/dL) is an independent predictor of mortality and readmission in heart failure patients.
Protein, Total
Abnormally high levels of protein in urine can be indicative of kidney disease.
Calcium
Impaired kidney function disrupts calcium-phosphate homeostasis, typically causing hypocalcemia due to decreased vitamin D activation and phosphate retention. Calcium monitoring is crucial for CKD-mineral bone disorder management.
Carbon Dioxide
Low levels of carbon dioxide in the blood can indicate a metabolic disorder, such as metabolic acidosis, where the body produces too much acid or doesn't get rid of enough acid.
Creatinine
ATN from ischemia or nephrotoxins causes tubular cell death and kidney dysfunction, resulting in rapid creatinine elevation. Creatinine levels help diagnose ATN and monitor recovery of kidney function.
Urea Nitrogen (Bun)
High levels of urea nitrogen (BUN) can indicate kidney disease or dehydration, as this waste product is filtered out of the blood by the kidneys.
Glucose
High levels of glucose can indicate diabetes, a chronic condition where the body's ability to process sugar is impaired.
eGFR
A low eGFR (estimated glomerular filtration rate) can indicate kidney disease, as this measures how well the kidneys are filtering waste from the blood.
Chol/Hdlc Ratio
A high Chol/Hdlc ratio indicates a higher risk of heart disease. The higher the ratio, the higher the risk.
LDL Cholesterol
This rare genetic disorder results in extremely low or absent LDL cholesterol due to inability to produce apoB-containing lipoproteins. Very low LDL-C (<20 mg/dL) with fat malabsorption suggests this diagnosis.
Triglycerides
Mutations in APOA5 gene cause severe hypertriglyceridemia. Genetic testing typically prompted by extreme triglyceride elevations. Triglycerides are primary monitoring parameter.
HDL Cholesterol
Mutations in APOA1 gene cause severe HDL deficiency (<10 mg/dL) with increased atherosclerosis risk. Very low HDL with absent or dysfunctional apoA-I is diagnostic of this rare genetic condition.
Cholesterol, Total
This is characterized by high levels of cholesterol in the blood, increasing the risk of heart disease.
Non HDL Cholesterol
High levels of non-HDL cholesterol can indicate an increased risk of cardiovascular disease as it represents all of the 'bad' cholesterol.
Lactic Acid, Plasma
Some cancers can increase lactic acid production, resulting in elevated plasma lactic acid levels.
Amylase
Amylase levels often rise 4 to 6 hours after onset of acute pancreatitis and remain elevated for several days. High levels of amylase in the blood can be an indication of this condition.
Creatine Kinase, Total
Alcoholism and drug abuse can lead to muscle damage, which can be detected by elevated Creatine Kinase levels.
GGT
Elevated levels of GGT are often found in individuals with alcohol use disorder, as the liver attempts to compensate for the damage caused by excess alcohol consumption. High GGT levels can be an early marker of this condition.
LD
Acute pancreatitis can lead to elevated LDH levels as the enzyme is released from damaged pancreatic cells into the bloodstream.
Magnesium
Low levels of magnesium can trigger bronchoconstriction and provoke asthma attacks. Magnesium helps in relaxing the bronchial muscles and regulating breathing.
Phosphate (As Phosphorus)
Chronic Kidney Disease can cause high phosphate levels in the blood, as the kidneys are less able to eliminate excess phosphate. This leads to Hyperphosphatemia.
Uric Acid
This is a disorder of the kidney's function in which substances like glucose and amino acids are passed in the urine instead of being reabsorbed by the kidneys. It can lead to low levels of uric acid in the blood.
Three steps from order to answer
Order online
Purchase securely on this page. Choose your nearest Quest Diagnostics draw site at checkout. Over 2,200 locations nationwide.
Takes about 2 minutes
Get your blood drawn
Book a time at your chosen location. A standard blood draw takes about 5 minutes. Your lab order is sent automatically when you purchase.
About 5 minutes at the lab
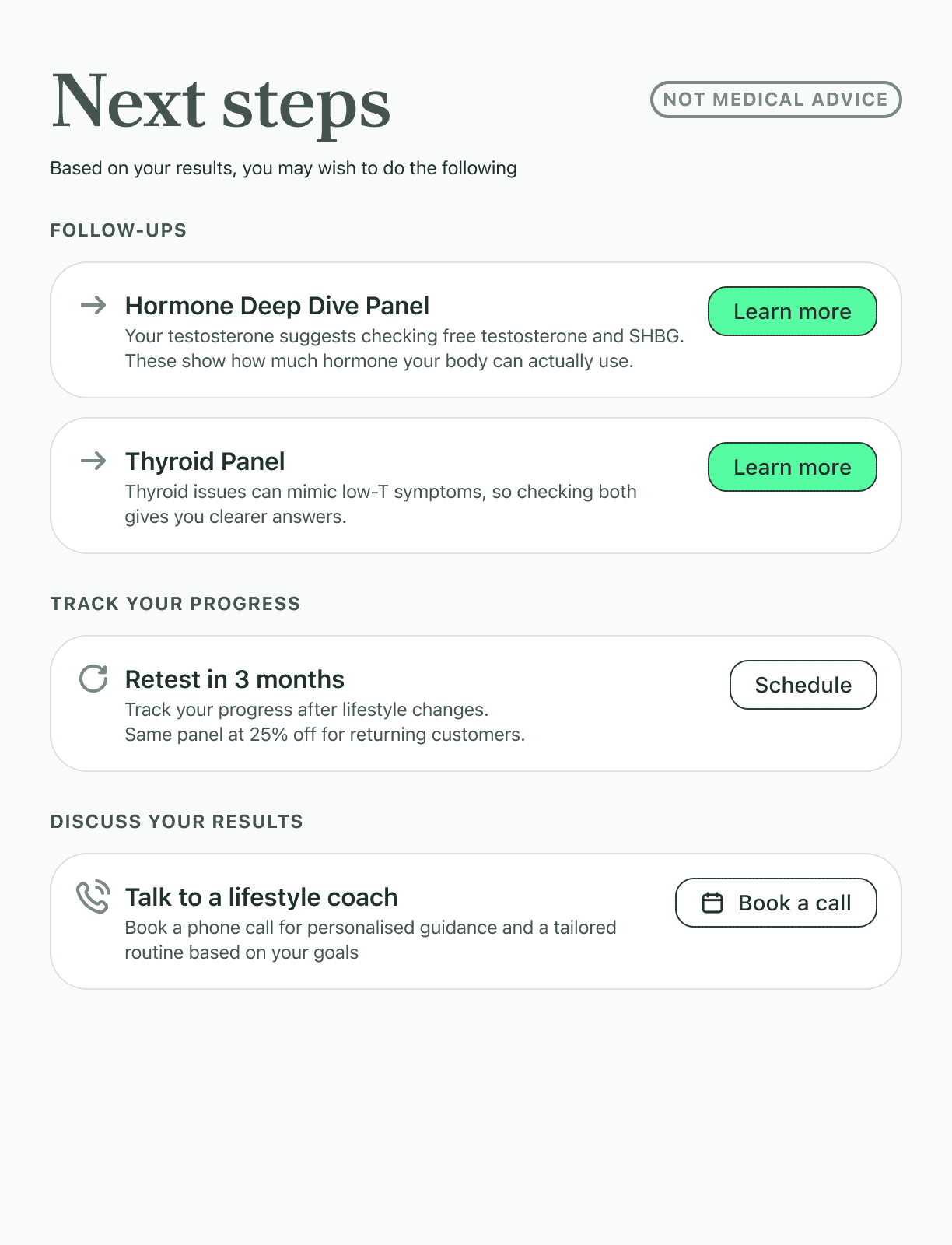
Review your results
Results arrive in your secure online portal in 1 to 2 business days. Each marker includes a plain-English explanation and reference range, not just a number.
Results in 1 to 2 business days
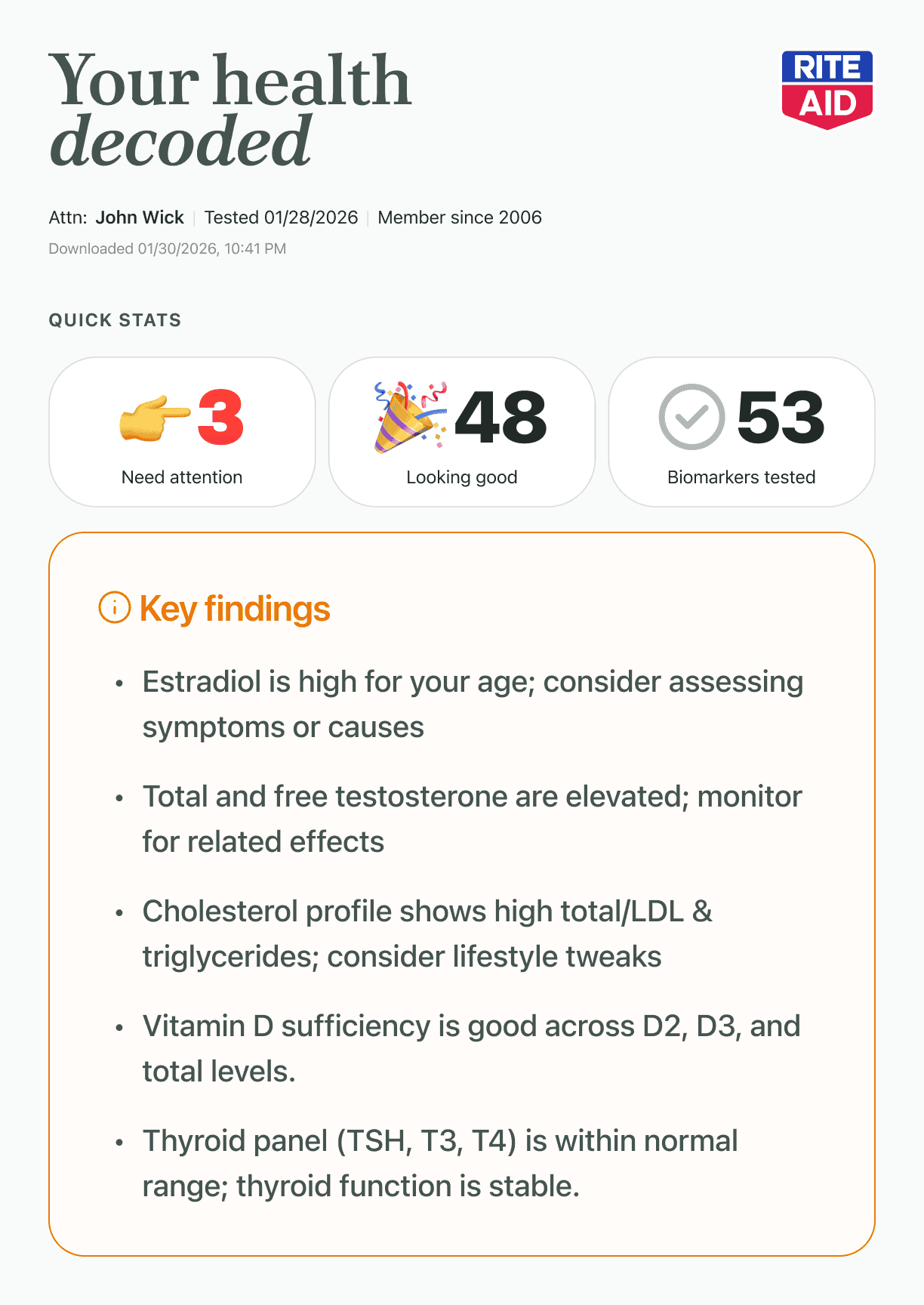
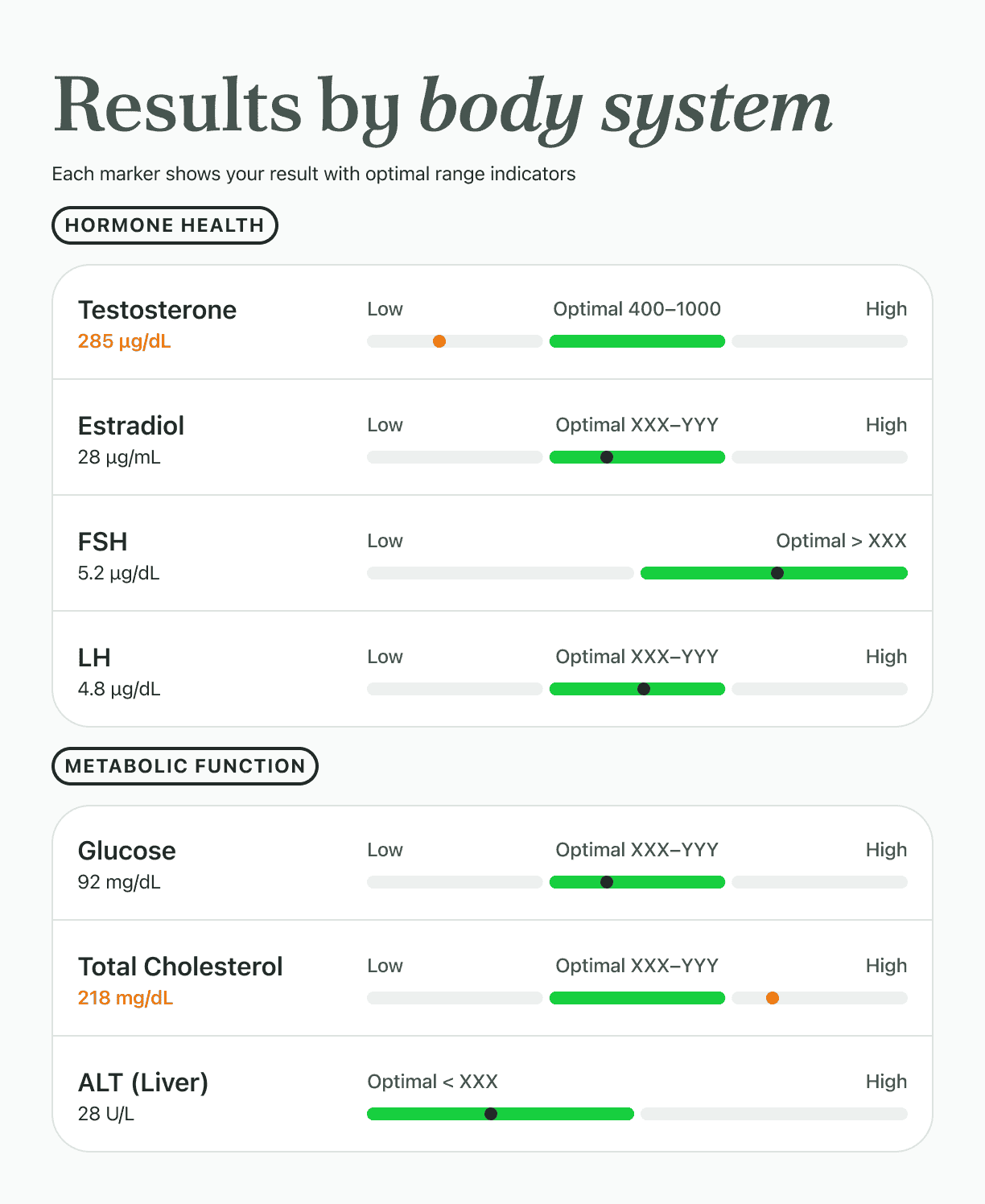
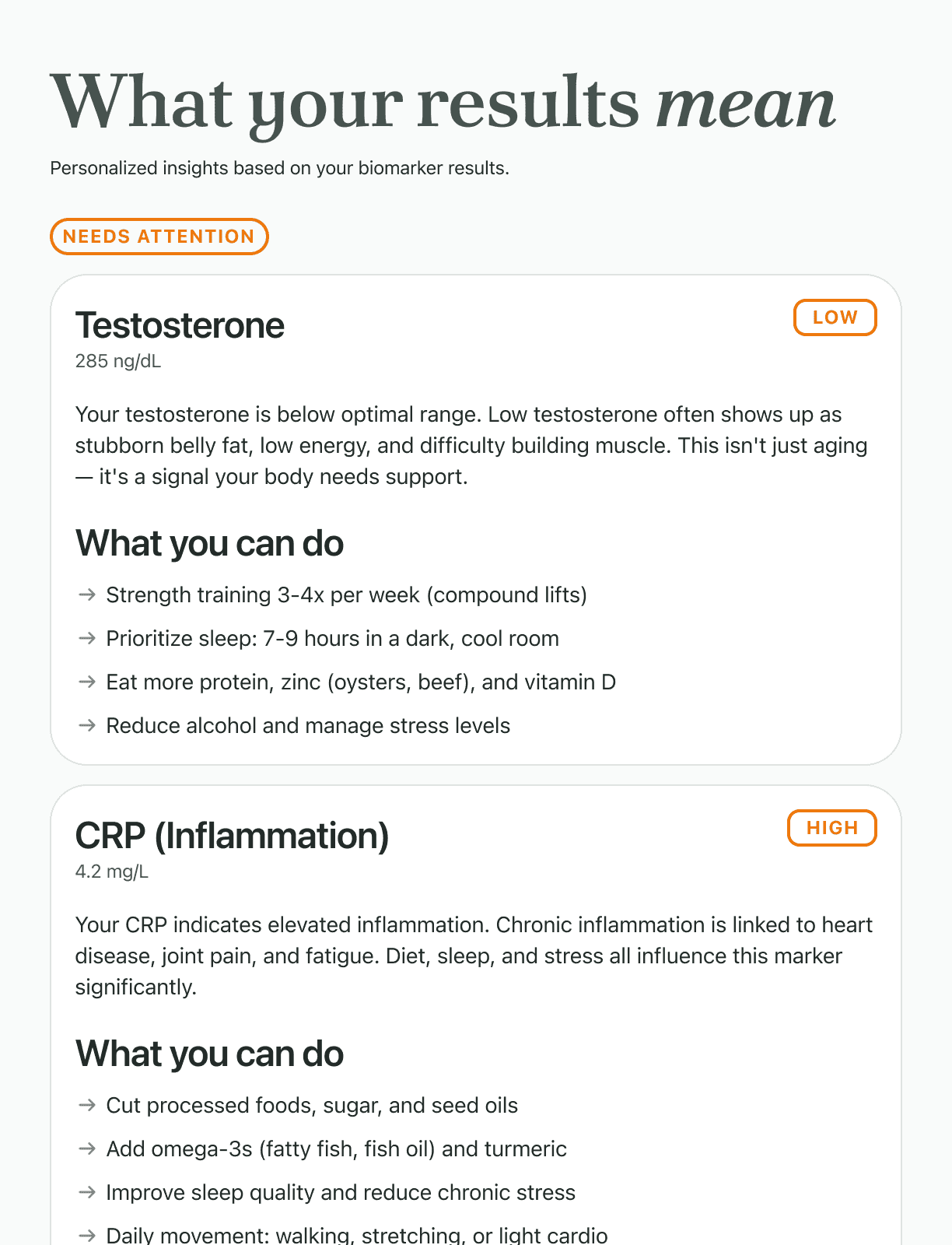
Results you can actually read.
Your results aren't just a number in a table. Each marker comes with a plain-English explanation and your result highlighted against the reference range. If anything falls outside normal, you'll see a note on what that typically means.
- Reference ranges shown for every marker
- Plain-English explanations, not medical jargon
- Downloadable as a PDF to share with your doctor
- Reviewed by a licensed physician before delivery
Results
what your report will look like

What makes this different from a standard doctor's visit
No doctor's visit required
All tests are physician-ordered on your behalf. You get clinical-grade diagnostics without a referral or prior appointment.
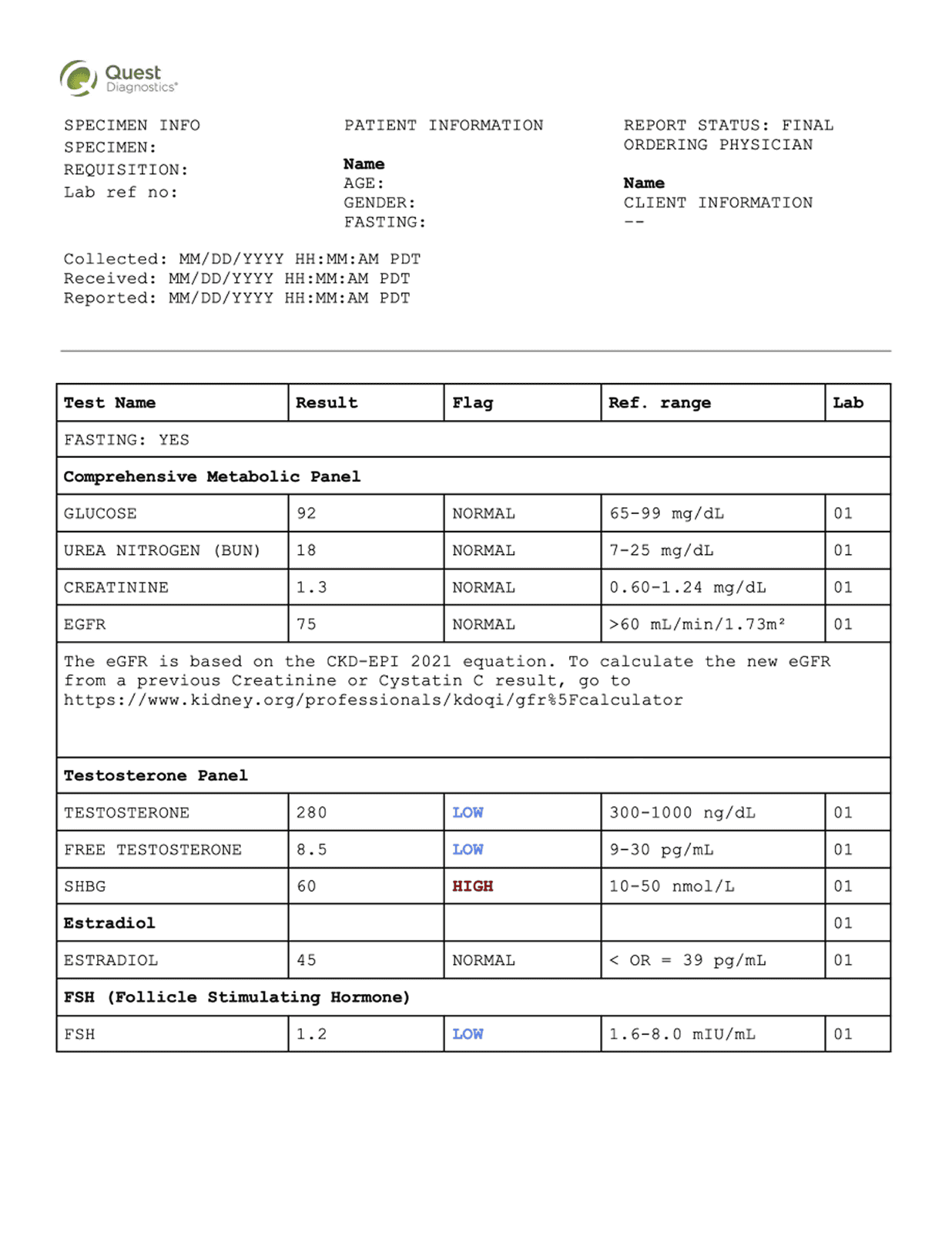
The same labs your doctor uses
Every blood draw is processed at Quest Diagnostics. The same facilities hospitals and clinics use nationwide. The science is identical. The experience is simpler.
Your results, your data
Results are private and belong to you. Download them, share with your own doctor, or keep them confidential. The choice is yours.
Physician-reviewed results
A licensed physician reviews your panel before results are released to you. If critical values are found, you'll be contacted directly.
Frequently asked questions
Text us at 863-270-9911 and we'll respond within a few hours.
No. When you purchase this test, a physician associated with our network reviews your order and issues the lab requisition on your behalf. You don't need a prior doctor's visit or referral.
This is a direct-pay test, priced to be accessible without insurance. Because you're paying directly, the cost is often lower than your insurance copay for a comparable physician-ordered panel. We provide an itemized receipt you can submit for HSA/FSA reimbursement.
The blood draw process and lab analysis are identical. Same CLIA-certified Quest Diagnostics facilities, same testing methodology. The difference is access. You order directly, skip the office visit, and get results faster.
A licensed physician reviews every panel before results are released. If any critical values are found, you'll receive a direct phone call before your results are posted. For out-of-range results that aren't critical, your results will include clear guidance on what the finding typically means and what next steps to consider.
Yes. Results are available as a PDF download from your portal. They're formatted in the standard lab report format your physician will recognize. Many people use these results to have a more informed conversation at their next appointment.
Your results are stored securely in a HIPAA-compliant system and are not shared with your insurance company, employer, or any third party without your explicit consent.